The of Arch Of Foot
The arches are shaped by the metatarsal and tarsal bones and braced by tendons and ligaments of the foot.
Arches are supported by intrinsic and extrinsic muscles of the sole in addition to ligaments, aponeurosis and shape of the bones.
Foot prints are not complete due to the arches The foot has to suffer from many disorders because of tight shoes or high heels which one wears for various reasons
arches of the foot help in fast walking, running /land jumping In addition, these help weight-bearing and in providing upright posture the foot is really unique to human being.
Introduction
The foot has to act
1) as a pliable platform to support the body weight in the upright posture, and
2) as a lever to propel the body forwards in walking, running or jumping. To meet these requirements, the human foot is designed in the form of elastic arches or ' springs. These arches are segmented, so that they can best sustain the stresses of weight and of thrusts. The presence of the arches makes the sole concave. This is best appreciated by examining foot prints which show the weight-bearing parts of the sole
An arched foot is a distinctive feature of man. It distinguishes him from other primates. The arches are present right from birth, although they are masked in infants by the excessive amount of fat in their soles.
CLASSIFICATION OF ARCHES
A. Longitudinal 1. Medial 2. Lateral
B. Transverse 1. Anterior 2. Posterior
Right foot print that showing the weight bearing point of sole

FORMATION OR STRUCTURE OF ARCHES
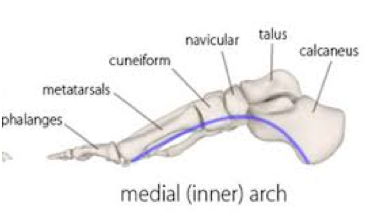
Medial Longitudinal Arch
This arch is considerably higher, more mobile and resilient than the lateral. Its constitution is as follows.
Ends: The anterior end is formed by the heads of the first, second and third metatarsals. The phalanges do not take part in forming the arches. The posterior end of this arch is formed by the medial tubercle of the calcaneum
Summit: The summit of the arch is formed by the superior articular surface of the body of the talus.
Pillars: The anterior pillar is long and weak. It is formed by the talus, the navicular, the three cuneiform bones, and the first three metatarsal bones. The posterior pillar is short and strong. It is formed by the medial part of the calcaneum .
The main joint of the arch is the talocalcaneonavicular joint.
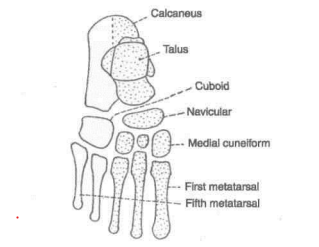
Bone forming the arches of foot ,.Superior View
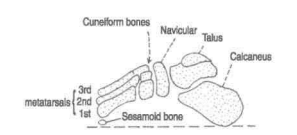
Bone Forming the arche of foot medial view
Lateral Longitudinal Arch
This arch is characteristically low has limited mobility and is built to transmit weight and thrust to the ground this is an contrast to the medial longitudinal arch which is act as a shock absorber the constitution of the lateral longitudinal arch is follow
End - The anterior end of arch is formed by the head of the 4th and 5th metatarsal bone
The posterior end is formed by the lateral tubercle of the Calcaneum
Summit - the Summit lies at the level of the articular facet on the superior surface at the Calcaneum at the level of the Subtalar joint
Pillar - the anterior pillar is long and weak , it is formed by the cuboid bone and by the 4ht and 5th metatarsal and the poetrior pillar is short and strong ,it is formed by the lateral half of Calcaneum
Main Joint: The main joint of the arch is the calcaneocuboid joint.

Anterior Transverse Arch
The anterior transverse arch is formed by the heads of the five metatarsal bones. It is complete because the heads of the first and fifth metatarsals both come in contact with the ground, and form the two ends of the arch
The dome-shaped transverse arch is elevated medially across the tarsal bones at the tarsometatarsal joints and held in place by the tarsometatarsal ligament
Posterior Transverse Arch
The posterior transverse arch is formed by the greater parts of the tarsus and metatarsus. It is incomplete because only the lateral end comes in contact with the ground, the arch forming a 'half dome' which is completed by a similar half dome of the opposite foot.
FACTORS RESPONSIBLE FOR MAINTENANCE OF ARCHES
In general, the factors helping in maintaining the various arches are as follows.
1. Shape of the bones concerned.
2. Intersegmental ties or ligaments (and muscles) that hold the different segments of the arch together. I
3. Tie beams or bowstrings that connect the two ends of the arch.
4. Slings that keep the summit of the arch pulled up. Each of these factors is considered below
1 J. Bony Factor
The posterior transverse arch is formed, and maintained mainly because of the fact that many of the tarsal bones involved (e.g., the cuneiform bones), and the heads of the metatarsal bones, are wedge-shaped, the apex of the wedge pointing downwards. The bony factor is not very important in the case of the other arches.
2. Intersegmental Ties
All arches are supported by the ligaments uniting the bones concerned. The most important of these are as follows.
(i) The spring ligament for the medial longitudinal arch .
(ii) The long and short plantar ligaments for the lateral longitudinal arch
(iii) In the case of the transverse arch, the metatarsal bones are held together by the interosseous muscles also

H Beams
The longitudinal arches are prevented from flattening by the plantar aponeurosis, and by the muscles of the first layer of the sole. These structures keep the anterior and posterior ends of these arches pulled together. In the case of the transverse arch, the adductor hallucis acts as a tie beam
. Slings
(a) The summit of the medial longitudinal arch is pulled upwards by tendons passing from the posterior compartment of the leg into the sole, i.e. tibialis posterior, flexor hallucis longus, flexor digitorum longus

Tendon supporting the medial longitudinal arch of foot
(b) The summit of the lateral longitudinal arch is pulled upwards by the peroneus longus and peroneus brevis (c) The tendons of the tibialis anterior and the peroneus longus together form a sling (or stirrup) which keeps the middle of the foot pulled upwards, thus supporting the longitudinal arches. (d) As the tendon of the peroneus longus runs transversely across the sole, it pulls the medial an

Plantar ligament that help to support the lateral longitudinal arch of foot

lateral margins of the sole closer together, thus maintaining the transverse arches. The transverse arch is also supported by the tibialis posterior which grips many of the bones of the sole through its slips
Function of Arches
1. The arches of the foot distribute body weight to the weight-bearing areas of the sole, mainly the heel and the toes. Out of the latter, weight is borne mainly on the first and fifth toes. The lateral border of the foot bears some weight, but this is reduced due to the presence of the lateral longitudinal arch
2. The arches act as springs (chiefly the medial longitudinal arch) which are of great help in walking and running
3. They also act as shock absorbers in stepping and particularly in jumping
4. The concavity of the arches protects the soft tissues of the sole against pressure.
CLINICAL ANATOMY ( APPLIED Anatomy )
1. Absence or collapse of the arches leads to flatfoot
pes planus, which may be congenital or acquired. The effects of a flat foot are as follows,
(a) Loss of spring in the foot leads to a clumsy, shuffling gait,
(b) Loss of the shock absorbing function makes the foot more liable to trauma and osteoarthritis
(c) Loss of the concavity of the sole leads to compression of the nerves and vessels of the sole. Compression of the communication between the lateral and medial plantar nerves causes neuralgic pain in the forefoot (meta-tarsalgia). Compression of blood vessels may cause vascular disturbances in the toes.
2. Exaggeration of the longitudinal arches of the foot is known as pes cavus. This is usually a result of contracture (plantar flexion) at the transverse tarsal joint.
When dorsiflexion of the metatarsophalangeal joints, and plantar flexion of the interphalangeal joints (due to atrophy of lumbricals and interossei) are superadded, the condition is known as claw-foot
The common causes of pes cavus and claw-foot are spina bifida and poliomyelitis.
. Other deformities of the foot are as follows.
(a) Talipes equinus in which the patient walks on toes, with the heel raised;
(b) talipes calcaneus in which the patient walks on heel, with the forefoot raised
;
(c) talipes varus in which the patient walks on the outer border of foot (foot is inverted and adducted); and
(d) talipes valgus in which the patient walks on the inner border of foot (foot is everted and abducted)
The commonest deformity of the foot is talipes equino varus (or club foot). In this condition the foot is inverted, adducted and plantar flexed. The condition may be associated with spina bifida.
1 What are the 3 types of foot arch?
The medial longitudinal arch, the lateral longitudinal arch, and the anterior transverse arch are the three arches of the human foot. These arches are shaped by the metatarsal and tarsal bones and braced by tendons and ligaments of the foot
2 Why is foot arch important?
The arch provides the foot with the stiffness necessary to act as a lever that transmits the forces generated by leg muscles as they push against the ground. The arch also retains sufficient flexibility to function like a spring to store and then release mechanical energy
3 What is a normal foot arch?
Normal arch (medium)
If the middle part of your arch is about half filled, this means you have a normal arch. Your arch naturally supports your body weight and pronates, or rolls in, under a normal load. Look for shoes with firm midsoles and straight to semi curved lasts
4 Is having an arched foot good?
Their stiffer design doesn't allow the foot to roll enough to properly distribute weight under pressure. As a result, feet with a raised midfoot are more prone to injuries like hammertoes, calluses, corns, metatarsalgia, sesamoiditis, plantar fasciitis, and even ankle and Achilles tendon problems.
5 How can I improve my foot arch?
Stair arch raises
Slowly lift your right heel as high as you can, focusing on strengthening your arch. Rotate your arch inward as your knee and calf rotate slightly to the side, causing your arch to become higher. Slowly lower back down to the starting position. Do 2–3 sets of 10–15 repetitions on both sides
6 What does arch pain feel like?
Arch pain can be the result of one or a combination of conditions that develop in the sole of the foot. Patients will often describe a tightness, pulling, strain, burning or ripping sensation through the mid arch of the foot, in front of the heel but behind the ball of the foot.
7 Can foot arch be improved?

Yes. It is important to stretch and strengthen your foot arch muscles with these effective arch support exercises and foot strengthening exercises: Towel Curl: One of the easiest flat foot exercises is known as a towel curl.
8 Does foot arch pain go away?
When you have plantar fasciitis, you usually feel pain in the bottom of the heel or the arch of the foot. Some people describe the pain as feeling like a bruise or an ache. The pain tends to gradually go away once you begin walking around. With continued walking, the pain may return, but usually goes away after rest.
Writen and edit by
Dr.Akshay Raj Chandra
Consultant Physiotherapist
Ph +917827068869
credit
sir b.d chuarasia and other offocial book and site
note ;-please drop a mail for credit and removal . rajchandrapt09@gmail.com
Comments